A female with SCA (HbSS) presented at six years-of-age with acute and chronic bilateral ischemic strokes (right>left frontoparietal lobes) in the setting of bacterial meningitis. Despite chronic red cell exchange therapy for secondary stroke prevention, she developed new cerebral infarctions, which has previously been documented in patients with sickle cell disease and vasculopathy.8 At age 13 years, she developed bilateral moyamoya vasculopathy with occlusions of the internal carotid artery (ICA) terminus bilaterally, as well as M1 and A1 partial occlusion and lenticulostriate artery enlargement. She subsequently underwent right and left indirect surgical revascularization with encephaloduroarteriosynangiosis at age 14 and 15 years, respectively, and demonstrated clinical stabilization. She continued to receive monthly exchange transfusions for many years (Figure 1).
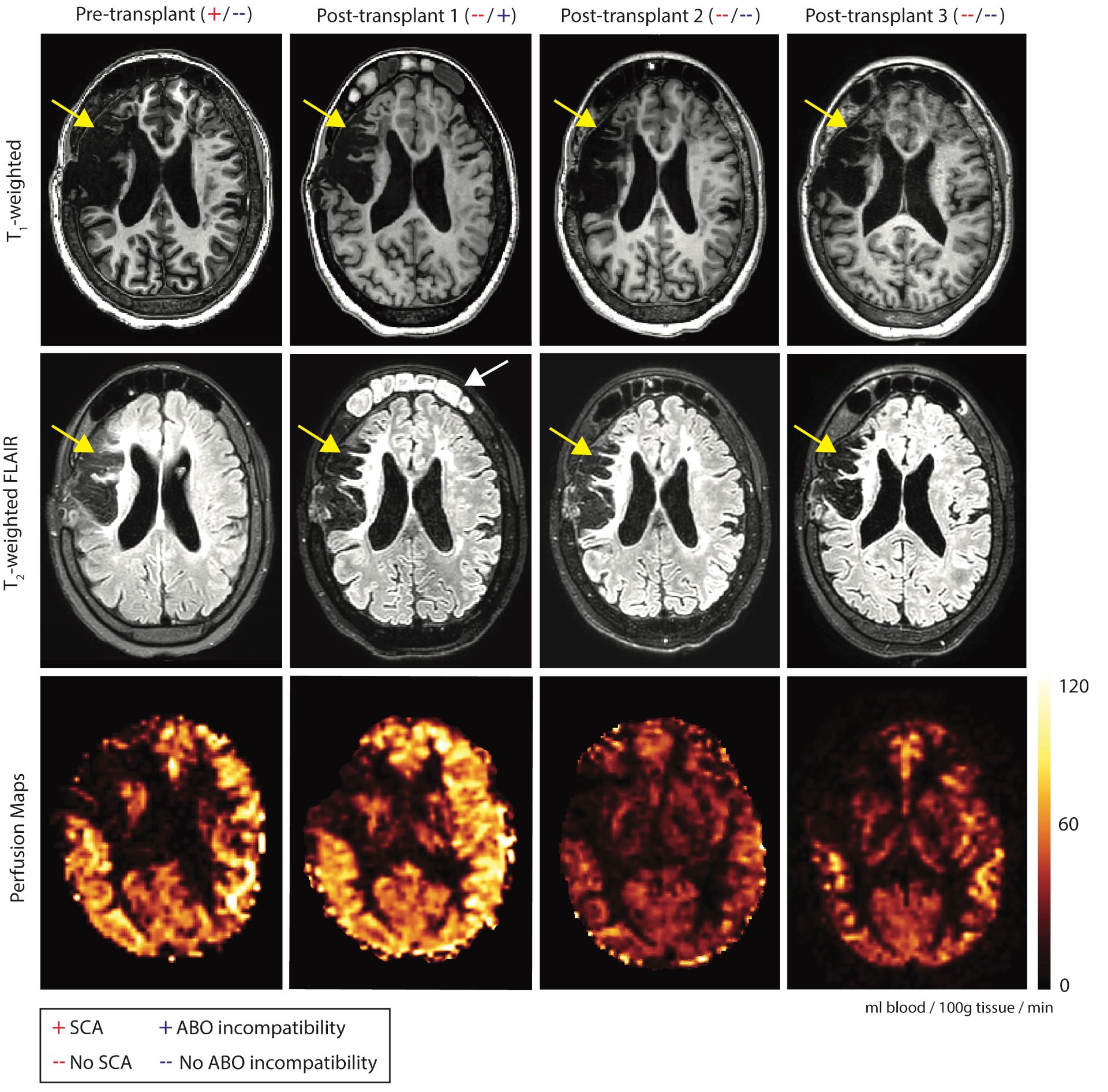
Figure 1
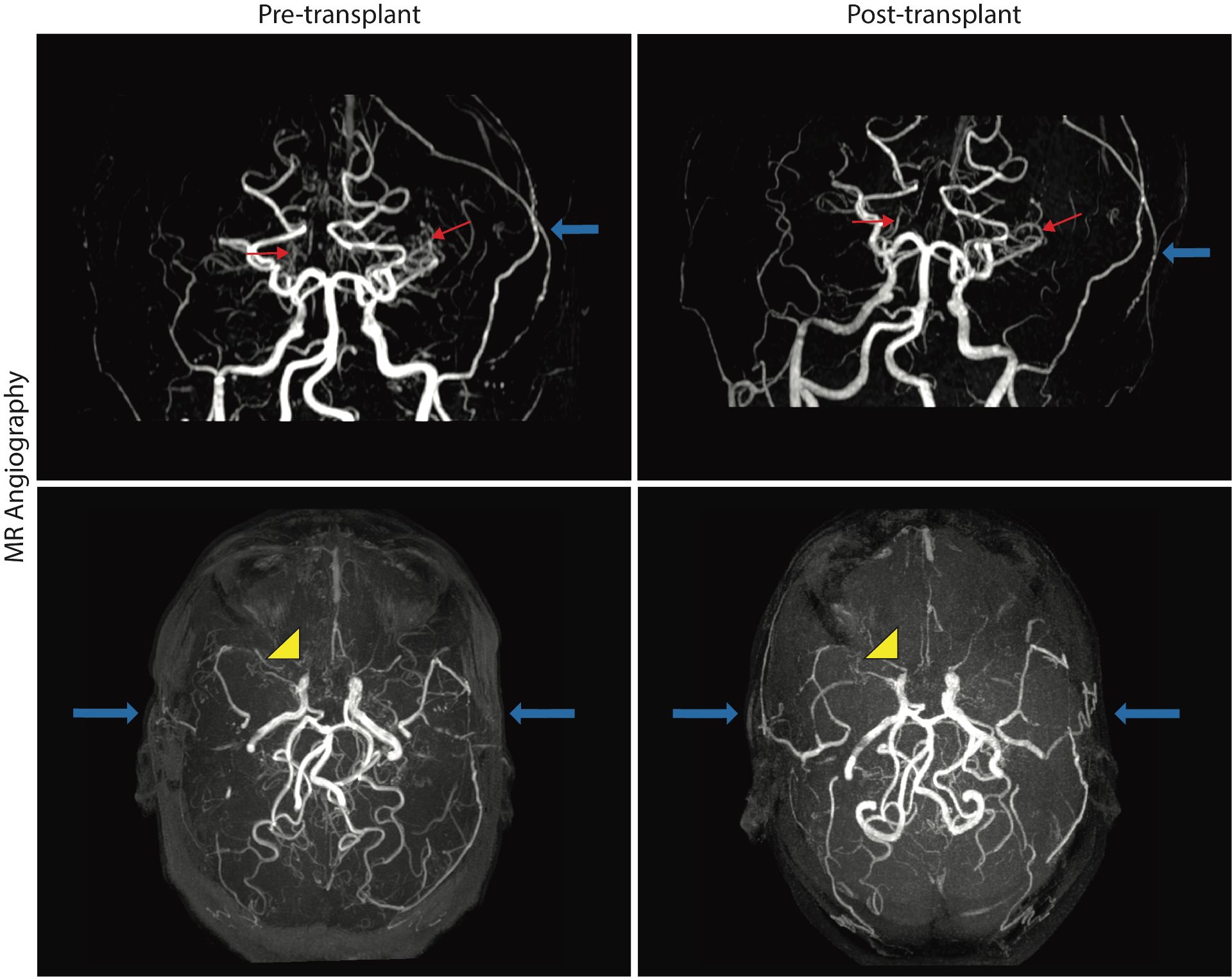
In her 20s, HSCT was recommended as curative treatment and was approved on an institutional transplant protocol due to stroke and MMS progression risk, and transfusion iron overload despite chelation. A non-myeloablative haploidentical bone marrow transplant (haplo-BMT) was prescribed, as the patient had no matched sibling and poor unrelated donor options. Her brother was identified as a haplo-match and served as the donor, with phenotype HbAA ABO blood type B+, while the patient was O+. Prior to HSCT, the patient underwent a MRI of the brain, including pseudocontinuous arterial spin labeling (pCASL) perfusion9 and oxygen extraction fraction (OEF)10 imaging. Pre-transplant, chronic left and right frontoparietal infarcts were noted, along with large areas of encephalomalacia in the middle cerebral artery distribution bilaterally. MR angiography was unchanged from prior studies. The patient’s hematocrit was 30%, with a moderately-elevated cortical CBF of 66.2 ml/100g/min in non-infarcted tissue and approximately normal OEF of 31.8%.
While engraftment was successful (HbAA genotype, 100% donor), the patient developed pure red cell aplasia (PRCA) related to the ABO incompatible HSCT, an autoimmune issue resulting in transfusion-dependent anemia. At this first post-transplant timepoint, the patient’s hematocrit was maintained at 25% with transfusion support. The patient’s CBF rose to 75.8 ml/100g/min with persistent anemia, and her OEF increased to 39.3%. No new infarcts were noted at this time, but cerebral hemodynamic measures remained concerning.
To address her PRCA and need for ongoing blood transfusions, the patient received two rituximab infusions, which were ineffective. She was subsequently given weekly injections of daratumumab 1800 mg for four weeks, which successfully treated her PRCA.11 Her hematocrit rose to 39%, within a normal range [36-48% in women],12 and has been maintained without transfusions. Correspondingly, CBF largely normalized to 38.2 ml/100g/min [normal range = 40-65 ml/100g/min],13,14,15 and the patient’s OEF was assessed at 36.3% [normal range = 35-45%].16 At a fourth timepoint, approximately three years post-transplant, cerebral hemodynamic measures remained stable, with hematocrit=41%, CBF=46.3 ml/100g/min, and OEF=40.4%. Overall, from pre-HSCT to post-HSCT after treatment for ABO incompatibility, the patient’s hematocrit increased, CBF normalized to an approximately healthy value (Figure 2), and OEF adjusted slightly, albeit within a normal range. No new strokes or silent cerebral infarcts have developed, and her cerebral vasculopathy remains severe but is stable at three years post-transplant (Figure 3).