Technical Report
Zachary T. Lowery1, Owen Chandler1, Thomas L. Wilson, MD1, Patrick A. Brown, MD1,2
1Department of Neurological Surgery, Wake Forest Baptist Medical Center, Winston-Salem, NC
2Department of Radiology, Wake Forest Baptist Medical Center, Winston-Salem, NC
Copyright © belongs to author(s)
All rights reserved.
Any redistribution or reproduction of part or all of the contents in any form is prohibited other than the following:
- you may print or download to a local hard disk extracts for your personal and non-commercial use only
- you may copy the content to individual third parties for their personal use, but only if you acknowledge the website as the source of the material
You may not, except with our express written permission, distribute or commercially exploit the content. Nor may you transmit it or store it in any other website or other form of electronic retrieval system.
Background
Pediatric emergent large vessel occlusion (ELVO) strokes are uncommon, but with the recent successes in interventional management of adult ELVO, interest in interventional management of pediatric presentations has increased.1 Several factors complicate the evaluation and management of pediatric stroke patients when compared to their adult counterparts. The etiologies of strokes in children typically vary from those in adults. Risk factors in children include cardiac disorders, vascular abnormalities, prothrombotic states, acute and chronic head and neck pathology, and infections, among others.2 Children may possess multiple simultaneous risk factors, further complicating their presentations. Additionally, because of the perceived rarity of pediatric stroke and hesitancy to perform CT angiographic evaluation, diagnosis is often delayed. Here we present the case of a 12-year-old male patient with history of transposition of the great vessels and arterial switch procedure who suffered an acute embolic stroke, was diagnosed with CT angiography (CTA), and underwent successful endovascular mechanical thrombectomy. Our case illustrates key commonalities as well as important differences between management of adult and pediatric emergent large vessel occlusion (ELVO).
Clinical Presentation
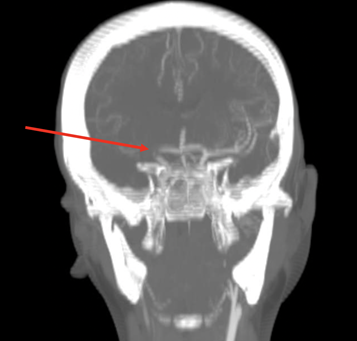
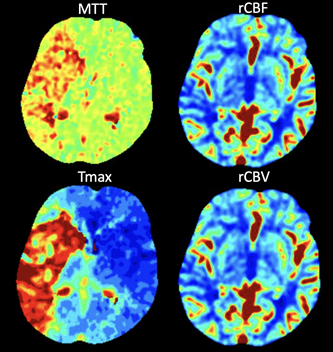
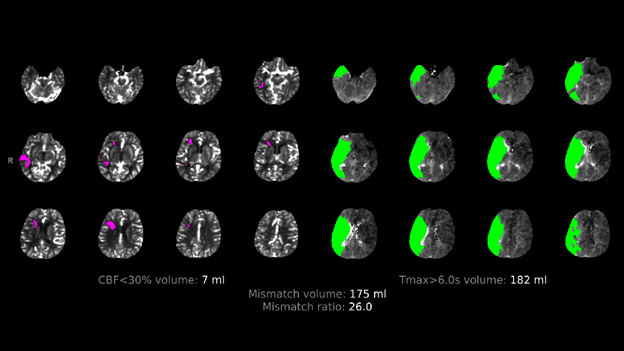
A twelve-year-old male patient with history of transposition of the great vessels and arterial switch procedure, ventricular septal defect (VSD), atrial septal defect (ASD), and left ventricular thrombus presented to the pediatric emergency department with left facial droop and left hemiparesis with initial National Institute of Health stroke scale (NIHSS) of 13. Time of onset was uncertain. Initial computed tomographic angiography (CTA) revealed an occlusive thrombus within the right internal carotid artery (ICA) terminus (Figure 1). CT perfusion (CTP) (RAPIDTM, iSchemaview, Inc., Menlo Park, CA) imaging predicted 175 mL penumbra and 7 mL core infarct (Figure 2, 3).
Treatment
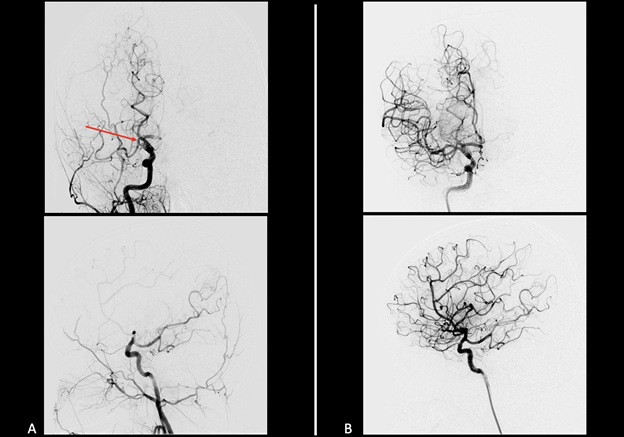
The patient was taken for endovascular thrombectomy under general anesthesia (Figure 4). Transfemoral approach (TFA) was chosen with 6-French short sheath and guide catheter, with initial contact aspiration followed by stent retriever-assisted aspiration techniques used to achieve modified thrombolysis in cerebral infarct (mTICI) grade 2c reperfusion3 after initial contact aspiration of the right ICA terminus with 5-French SofiaTM (Terumo, Aliso Viejo, CA) access catheter and subsequent rescue stent retriever-assisted suction aspiration thrombectomy of the right MCA with 5-French SofiaTM and 4 x 40 mm SolitaireTM (Medtronic, Dublin, Ireland). Immediately after the procedure, the patient was extubated and transferred to the pediatric ICU where his left-sided weakness substantially improved. He was subsequently transferred the same evening to a regional center where his congenital heart disease and ventricular thrombus were managed by his cardiac surgery and cardiology teams. At two weeks post-thrombectomy the patient was without neurologic deficit and had returned to baseline.
Discussion
We report the off-label use of the 5 French SofiaTM catheter and the SolitaireTM stent retriever device for mechanical thrombectomy in a pediatric patient with a complicated cardiac history. Our case highlights two major issues for consideration in the management of pediatric ELVO: nonstandard or off-label device use and pre-intervention imaging workup.
A recent review of 113 pediatric cerebral thrombectomy cases found technically successful reperfusion in 87.8% of cases.1 Still, the recent landmark randomized controlled trials demonstrating superiority of endovascular thrombectomy over standard medical care for ELVO strokes are based on adult data, and the tools that have been developed for treatment of these patients are designed and labeled for adult use.4 While currently available adult thrombectomy devices may be suitable for use in a wide range of ages in children, operators must be able to adapt and employ alternative devices and techniques when considering mechanical thrombectomy in the pediatric patient. Typical transfemoral (TFA) devices utilize 8-French platforms which may be too large for younger or smaller pediatric patients. In such cases, operators may consider utilizing an 8-French long sheath with TFA, enabling the advantages of a larger distal lumen without upsizing femoral access. In considering transradial access (TRA), most interventional platforms for stroke require 6- or 7-French access, which can be problematic for younger pediatric patients as a result of smaller arterial caliber and greater propensity for vasospasm. In a recent series of 47 cases of TRA for pediatric diagnostic and interventional neuroangiography, clinically significant vasospasm was noted in 13.1% of cases, and there was an 8.2% conversion rate to TFA.5 In time-sensitive procedures such as thrombectomy for ELVO, intraprocedural conversion to TFA may cost valuable time, which should be considered when contemplating TRA for pediatric stroke. Our case illustrates the successful transfemoral use of a 6-French access platform with off-label utilization of an intermediate access catheter for contact aspiration and stent retriever assisted contact aspiration thrombectomy. The above considerations highlight the need for operators caring for pediatric stroke patients to be adaptable to the unique challenges in this patient population and ready to consider alternative techniques when indicated.
CT angiography and CTP have developed into the mainstay imaging evaluations in emergent stroke imaging for adults. However, due to rarity of pediatric ELVO and confounding clinical presentations, MRI has continued to be a common primary imaging modality in acute pediatric neurologic presentations. Our case illustrates that when ELVO is a primary diagnostic consideration, particularly in the setting of known stroke risk factors such as complex congenital heart disease, thrombophilia, head and neck pathology, etc., CTA should be considered as a first-line imaging modality. When considering CTP in the emergent management of pediatric stroke, it is important to remember increased radiation exposure in these studies, and further potential diagnostic certainty should be balanced against radiation exposure risks.6 Because penumbral thresholds and definitions for core infarction may differ from adult values in the pediatric population,7 results from pediatric CTP evaluations should be analyzed cautiously. While CTP may be useful for pre-intervention evaluation in pediatric ELVO patients, particularly in delayed presentations, further studies are warranted for development of universal protocols to optimize these considerations. Institutional imaging protocols should be considered to prevent unnecessary delays in patient management when these cases arise.
Conclusion
Although pediatric ELVO remains an uncommon diagnosis, the unique challenges presented by pediatric patients may warrant the development of specific systems of imaging and intervention for this patient population. Interventionalists managing these patients should be able to apply techniques developed for the adult population but also ready to modify their approach to meet unique situations posed by younger pediatric patients. Imaging protocols should be tailored to clinical context, and when pediatric ELVO is a primary diagnostic consideration because of patient risk factors, CT and CTA should be considered a first-line imaging technique. While CTP may have some utility in evaluation pediatric stroke, particularly in delayed presentations, the need for diagnostic certainty should be weighed against radiation risks and potential confounding definitions of penumbral and core infarct thresholds in children. Finally, teams should consider development of pediatric-specific ELVO imaging and intervention protocols to optimize accuracy, timeliness, and safety of evaluation and treatment of these patients.
References
- Bhatia K, Kortman H, Blair C, et al. Mechanical thrombectomy in pediatric stroke: systematic review, individual patient data meta-analysis, and case series. J Neurosurg Pediatr. Published online August 9, 2019:1-14. doi:3171/2019.5.PEDS19126
- Mackay MT, Wiznitzer M, Benedict SL, et al. Arterial ischemic stroke risk factors: the International Pediatric Stroke Study. Ann Neurol. 2011;69(1):130-140. doi:10.1002/ana.22224
- Tung EL, McTaggart RA, Baird GL, et al. Rethinking Thrombolysis in Cerebral Infarction 2b: Which Thrombolysis in Cerebral Infarction Scales Best Define Near Complete Recanalization in the Modern Thrombectomy Era? Stroke 2017; 48:2488-2493.
- Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomized trials. Lancet 2016 Apr 23;387(10029):1723-31. Doi:10.1016/S0140-6736(16)00163-X.
- S. Food and Drug Administration. Center for Devices and Radiological Health. (2010). Initiative to Reduce Unnecessary Radiation Exposure from Medical Imaging. Washington, DC.
Lee S, Heit JJ, Albers GW. Neuroimaging selection for thrombectomy in pediatric stroke: a single-center experience. J Neurointerv Surg 2019; 11(9):940-946.
Endovascular Thrombectomy in Child w/Congenital Heart Disease