Case Report
Andy Cheuk-Him Ng1,3, Jeremy L Rempel2, Thilinie Rajapakse1, Janani Kassiri1, Janette Mailo1,3
1Division of Pediatric Neurology, Department of Pediatrics, University of Alberta, Edmonton, AB T6G 2R3, Canada; 2Department of Radiology, University of Alberta, Edmonton, Canada.
Corresponding Author: Andy Cheuk-Him Ng, University of Alberta
Copyright © belongs to author(s)
All rights reserved.
Any redistribution or reproduction of part or all of the contents in any form is prohibited other than the following:
- you may print or download to a local hard disk extracts for your personal and non-commercial use only
- you may copy the content to individual third parties for their personal use, but only if you acknowledge the website as the source of the material
You may not, except with our express written permission, distribute or commercially exploit the content. Nor may you transmit it or store it in any other website or other form of electronic retrieval system.
Introduction
The majority of ecstasy currently in use is composed of 3,4, methylenedioxymethamphetamine (MDMA). Although it is a derivative of amphetamine, it more closely resembles mescaline, a psychedelic protoalkaloid (1). The estimated number of worldwide users exceeds 22 million (2). While there is a clear association between cocaine and methamphetamine use with ischemic and hemorrhagic stroke, there is no epidemiology study looking at the incidence of stroke due to ecstasy use (3). At present, it is therefore unclear whether MDMA use increases the likelihood of stroke.
Case Report
A 17-year-old, right-hand dominant girl was evaluated in the emergency department at the Stollery Children’s Hospital, a tertiary care pediatric hospital with a catchment area of 2.2 million people. She had a history of major depressive disorder with psychotic features requiring electroconvulsive therapy eight months prior to presentation. Eleven months prior to admission, she started smoking marijuana at least three times per week, although the exact quantity is unknown. She takes no prescription medications. Eleven days prior to presentation, she used a total of 1.5 grams of ecstasy for the first time. Within 10 minutes, she experienced transient vertigo, and she described a new onset of blurriness of her “peripheral” vision, which was persistent. Two days later, she had a new onset occipital headache. She took 5- hydroxytryptophan (5-HT) supplements in an attempt to mitigate the headache, although it had no effect. Six days later, she experienced vague visuospatial complaints in the form of getting lost while walking home and being unable to recognize the colour coding on her school locker.
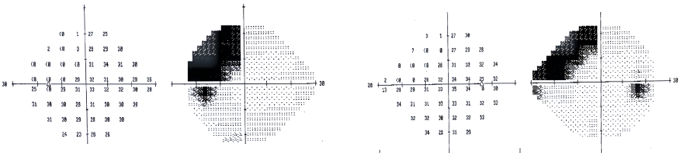
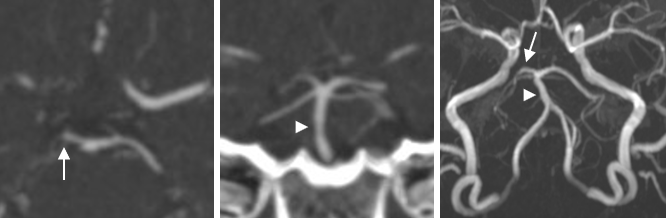
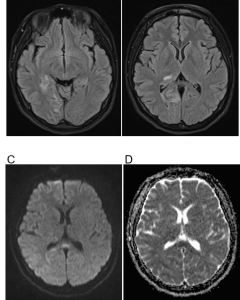
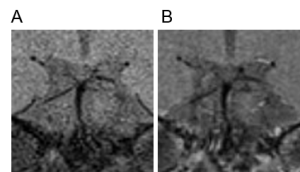
She presented to her local optometrist who discovered a left homonymous superior quandrantanopia (Figure 1). CT head and neck angiogram demonstrated an occlusion in the P1 segment of the right posterior cerebral artery and mild irregularity of the basilar artery (Figure 2). MRI brain showed T2/FLAIR hyperintensities in the subcortical region in the right dorsal thalamus, right medial parietal lobe, right hippocampus and parahippocampal gyrus with smaller areas of restricted diffusion in the same regions (Figure 3). These findings were in keeping with vasogenic edema and areas of subacute ischemic stroke. While in hospital, she was found by psychiatry to have a thought disorder characterized by tangential thought processes and pressured speech and new onset formed human-figured hallucinations in her left upper visual field. We were unable to determine the exact onset of her psychosis, and therefore, cerebral vasculitis was a possible differential diagnosis. CSF studies were unremarkable. EEG showed right posterior quadrant background slowing without epileptiform discharges. MRI brain vessel wall imaging demonstrated no vessel wall enhancement that is often seen in inflammatory conditions such angiitis of the CNS (Figure 4). The presumptive diagnosis was therefore reversible cerebral vasoconstriction syndrome (RCVS), and she was started on ASA with gradual improvement of her headache. She was transferred to pediatric psychiatry ward for her ongoing psychosis management with close pediatric neurology follow up. MRI time of flight angiogram performed eight weeks after her initial presentation showed marked improvement of the vasoconstriction in her basilar artery and right PCA occlusion (Figure 2C).
Discussion
We reported a pediatric patient with a chronic history of marijuana use who presented with RCVS and stroke immediately after a first-time ecstasy use. The close temporal association suggested that ecstasy played a critical factor in causing vasoconstriction, although 5-HT and the chronic marijuana use were also risk factors.
There have been several reports of ischemic stroke in the context of MDMA use in the adult literature. The first reported case of MDMA-associated stroke occurred in a 28 year old man with a left striatocapsular infarct (4). There were two additional cases of MDMA-associated
ischemic infarctions in the left MCA territory due to mild to moderate left distal internal carotid narrowing and focal beading and outpouching of left MCA, respectively (5, 6). Bilateral globus pallidus infarction has also been attributed to MDMA use in a 41 year old man, although the underlying mechanism was unclear (7). A ruptured right middle cerebral artery aneurysm causing subarachnoid hemorrhage was also seen in the context of MDMA use (8).
A recent retrospective observational study of 9350 patients showed no association between recent cannabis use and acute ischemic stroke (9). Another cross-sectional survey of 43860 patients showed a 1.82x higher odds of stroke compared to non-cannabis users (10). The history of marijuana use provided by our patient was obtained during a manic state and details surrounding her marijuana use is uncertain. Therefore, it is unclear if marijuana use played a role in our patient’s presentation.
MDMA blocks the reuptake of the monoamine neurotransmitters serotonin, norepinephrine, and dopamine (1). The acute psychoactive properties of MDMA are likely due to the accumulation of serotonin and possibly dopamine. At higher doses of MDMA, massive release of serotonin has been shown to cause psychosis and neuronal damage (11, 12). The mechanism of RCVS induced by MDMA is unclear but is postulated to be due to serotonin-mediated cerebral vasoconstriction (4-6). The degree of vasogenic edema and her persistent symptoms were likely exacerbated by 5-HT use, which is also a serotonergic agent.
Posterior circulation multifocal narrowing due to MDMA use has not been previously reported. In addition, this case highlighted the often-challenging clinical aspect of distinguishing between RCVS and angiitis of the central nervous system in the acute setting. We used the RCVS2 score to determine the likelihood of RCVS in our patient (13). She had an RCVS2 score of 4 (presence of vasoconstrictive trigger and female sex) and thus a specificity of 86 % for RCVS. However, an
RCVS2 score of 4 remains equivocal, as several conditions such as vasculitis, moyamoya, radiation, and atherosclerosis were also relatively common in the initial derivation cohort (13). In addition, RCVS2 score has not been validated in the pediatric population. In our patient, however, RCVS is highly likely due to the marked improvement of her vasoconstriction in the follow-up MRI time of flight angiogram, which tends to overestimate arterial narrowing. Given the presence of psychosis of unknown onset and the lack of a clear history of thunderclap headache, we felt that it was prudent to rule out CNS inflammation and angiitis with a lumbar puncture and novel MRI-based vessel wall imaging (14). This case highlights the dangers of
MDMA as a potential trigger of vasospasm of the posterior circulation, leading to functionally impairing ischemic infarcts in the young.
References
- H. Kalant, The pharmacology and toxicology of “ecstasy” (MDMA) and related drugs. CMAJ 165, 917-928 (2001).
- J. M. Lappin, G. E. Sara, Psychostimulant use and the brain. Addiction 114, 2065-2077 (2019).
- A. C. Fonseca, J. M. Ferro, Drug abuse and stroke. Curr Neurol Neurosci Rep 13, 325 (2013).
- S. Hanyu, K. Ikeguchi, H. Imai, N. Imai, M. Yoshida, Cerebral infarction associated with 3,4-methylenedioxymethamphetamine (‘Ecstasy’) abuse. Eur Neurol 35, 173 (1995). 5. D. A. De Silva, M. C. Wong, M. P. Lee, C. L. Chen, H. M. Chang, Amphetamine-associated ischemic stroke: clinical presentation and proposed pathogenesis. J Stroke Cerebrovasc Dis 16, 185-186 (2007).
- C. D. Muntan, V. Tuckler, Cerebrovascular accident following MDMA ingestion. J Med Toxicol 2, 16-18 (2006).
- K. De Smet, M. De Maeseneer, Y. A. Talebian, T. Stadnik, J. De Mey, Bilateral globus pallidus infarcts in ecstasy use. JBR-BTR 94, 93 (2011).
- J. Auer, R. Berent, T. Weber, E. Lassnig, B. Eber, Subarachnoid haemorrhage with “Ecstasy” abuse in a young adult. Neurol Sci 23, 199-201 (2002).
- C. V. San Luis et al., Association between recent cannabinoid use and acute ischemic stroke. Neurol Clin Pract 10, 333-339 (2020).
- T. Parekh, S. Pemmasani, R. Desai, Marijuana Use Among Young Adults (18-44 Years of Age) and Risk of Stroke: A Behavioral Risk Factor Surveillance System Survey Analysis. Stroke 51, 308-310 (2020).
- G. A. Ricaurte, J. Yuan, U. D. McCann, (+/-)3,4-Methylenedioxymethamphetamine (‘Ecstasy’)-induced serotonin neurotoxicity: studies in animals. Neuropsychobiology 42, 5-10 (2000).
- B. P. Boot, I. S. McGregor, W. Hall, MDMA (Ecstasy) neurotoxicity: assessing and communicating the risks. Lancet 355, 1818-1821 (2000).
- E. A. Rocha, M. A. Topcuoglu, G. S. Silva, A. B. Singhal, RCVS2 score and diagnostic approach for reversible cerebral vasoconstriction syndrome. Neurology 92, e639-e647 (2019).
14. D. M. Mandell et al., Vessel wall MRI to differentiate between reversible cerebral vasoconstriction syndrome and central nervous system vasculitis: preliminary results. Stroke 43, 860-862 (2012).
MDMA Induced Cerebral Vasospasm