Case Report
Lasya Challa1, Wilmot Bonnet2, Kimberly Goodspeed2, Cory Pfeifer3
1 Division of Pediatric Hospital Medicine, Department of Pediatrics, University of Texas Southwestern Medical Center, Dallas, Texas
2 Division of Pediatric Neurology, Department of Pediatrics, University of Texas Southwestern Medical Center, Dallas, Texas
3 Department of Radiology, University of Texas Southwestern Medical Center, Dallas, Texas
Copyright © belongs to author(s)
All rights reserved.
Any redistribution or reproduction of part or all of the contents in any form is prohibited other than the following:
- you may print or download to a local hard disk extracts for your personal and non-commercial use only
- you may copy the content to individual third parties for their personal use, but only if you acknowledge the website as the source of the material
You may not, except with our express written permission, distribute or commercially exploit the content. Nor may you transmit it or store it in any other website or other form of electronic retrieval system.
Case Report
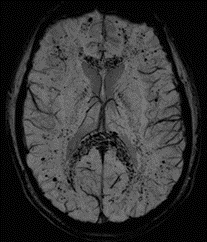
A 17-year-old, previously healthy male was admitted to the hospital with respiratory distress and malaise. He presented with a history of fever, body aches, chest pain, shortness of breath and cyanosis after failing outpatient flu treatment with Tamiflu. He was hypoxic (SpO2 49% on room air) and had bilateral reticulonodular opacities on chest X-ray. His infectious workup included testing for common bacterial and viral pathogens was negative. He had a 7-month history of vaping and urine toxicology screen was positive for Carboxy-delta 9-THC Glucuronide (THC), naproxen and opiates (given in ED). He was diagnosed with E-cigarette or vaping product use-associated lung injury (EVALI) and admitted to the ICU on positive pressure ventilation. He progressed to acute respiratory distress syndrome (ARDS) requiring intubation and mechanical ventilation. He developed microvascular and left ventricular thrombi with splenic and nephric infarcts requiring anticoagulation. He was started on an unfractionated Heparin drip and was then transitioned to Enoxaparin. Despite a normal neurologic exam, a brain MRI/MRA obtained 12 days after initiation of anticoagulation was notable with microembolic disease. MRA was normal.
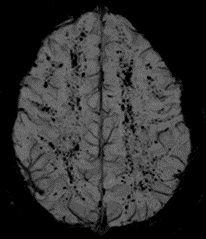
MRI Brain: Widespread microembolic thrombi with areas of restricted diffusion and signal voids on susceptibility-weighted imaging (SWI) throughout the brain, greatest in the splenium of corpus callosum and watershed regions.


Discussion
This patient has findings of diffuse cerebral microhemorrhages in the setting of EVALI-related respiratory failure. It remains unclear if imaging findings are related to thromboembolic events, severe lung injury, or is a manifestation of vaping-related toxicity. Notably, there was no apparent neurological deficit on bedside exam. Because he is at risk of deficits in cognitive functioning such as processing speed, memory, or executive function, he will undergo a neuropsychological evaluation.
Our patient’s story is similar to the case reported by Messina et al. in the Journal of Pediatric Radiology which involved a teen found to have restricted diffusion in the corpus callosum, which the authors noted was consistent with a cytotoxic lesion of the corpus callosum (CLOCC)1. There was, however, no mention of susceptibility weighted imaging and/or microhemorrhages related to the lesion in this case. Our case, then, adds to the variety of imaging findings possible with EVALI and reinforces the need for brain imaging in this population. Some have suggested that the involvement of the splenium of the corpus callosum in CLOCC may be due to loss of autoregulation and hypoxic vasodilation due to lack of adrenergic tone leading to overperfusion, which in turn, could contribute to the appearance of microhemorrhages2.
Other explanations for the findings on imaging were also considered. Cerebral fat embolism syndrome can have similar findings on imaging when droplets of marrow fat can embolize to the brain after a long bone or pelvic fracture via right-to-left shunting at the cardiac or pulmonary level. Similar to our patient, the fat emboli target the white matter and may be associated with confluent cytotoxic edema and petechial hemorrhage3,4. The pattern is also similar to prior reports from severe lung injury and high altitude lung injury5,6,7. In three ARDS survivors, brain MRI revealed multiple microhemorrhages, predominantly in the splenium of the corpus callosum, similar to our patient5. Possible mechanisms of injury include disruption of the blood-brain barrier due to a cytokine storm that allows for leakage of blood into the parenchyma, impaired venous return due to positive pressure ventilation, and hypoxia7. The widespread nature of the MRI findings on SWI in our patient are less consistent with clinically occult micro emboli from the cardiac thrombus.
The pathophysiology by which e-cigarette use results in brain damage remains elusive. One hypothesis is that the carrier agents used in these devices, such as Vitamin E acetate, may play a role. A synthetic form of Vitamin E acetate serves as a thickening agent embedded with THC-containing products8. Isotope dilution mass spectrometry methods developed by the CDC to analyze specific toxicants in fluid obtained from bronchoalveolar lavages (BAL) in 29 patients with EVALI showed Vitamin E acetate in all patient BAL samples providing direct evidence of vitamin E acetate at the primary site of injury and possibly the inciting agent8. Though causation has not been established, the MR findings observed in our patient may relate to subclinical cerebral micro emboli of the vitamin E acetate or other lipids used in vaping products. Further studies are needed to explore this relationship.
Here we describe a report of diffuse cerebral microhemorrhages found in the setting of severe lung injury in EVALI. The pattern of multiple microhemorrhages focused in the splenium of the corpus callosum is atypical and should be investigated as a potential biomarker in similar cases. Our case demonstrates the importance of neuroimaging in this population and the need for detailed neurologic and cognitive evaluation after EVALI.
References
- Messina MD, Levin TL, Blumfield E. Cytotoxic lesion of the splenium of the corpus callosum in a patient with EVALI. Clin Imaging. 2020;66:73-76. doi:10.1016/j.clinimag.2020.05.009
- Garcia-Monco JC, Cortina IE, Ferreira E, et al. Reversible splenial lesion syndrome (RESLES): what’s in a name?. J Neuroimaging. 2011;21(2):e1-e14. doi:10.1111/j.1552-6569.2008.00279.x
- Kuo KH, Pan YJ, Lai YJ, Cheung WK, Chang FC, Jarosz J. Dynamic MR imaging patterns of cerebral fat embolism: a systematic review with illustrative cases. AJNR Am J Neuroradiol. 2014;35(6):1052-1057. doi:10.3174/ajnr.A3605
- Yeap P, Kanodia AK, Main G, Yong A. Role of susceptibility-weighted imaging in demonstration of cerebral fat embolism. BMJ Case Rep. 2015;2015.
- Riech S, Kallenberg K, Moerer O, et al. The Pattern of Brain Microhemorrhages After Severe Lung Failure Resembles the One Seen in High-Altitude Cerebral Edema. Crit Care Med. 2015;43(9):e386-e389. doi:10.1097/CCM.0000000000001150
- Hall JP, Minhas P, Kontzialis M, Jhaveri MD. Teaching NeuroImages: Distinct brain microhemorrhage pattern in critical illness associated with respiratory failure. Neurology. 2018;90(22):e2011. doi:10.1212/WNL.0000000000005609
- Hackett PH, Yarnell PR, Weiland DA, Reynard KB. Acute and Evolving MRI of High-Altitude Cerebral Edema: Microbleeds, Edema, and Pathophysiology. AJNR Am J Neuroradiology. 2019;40(3):464-469. doi:10.3174/ajnr.A5897
- Blount BC, Karwowski MP, Shields PG, et al. Vitamin E Acetate in Bronchoalveolar-Lavage Fluid Associated with EVALI. N Engl J Med. 2020;382(8):697-705. doi:10.1056/NEJMoa1916433
- Liebeskind DS, Sanossian N, Sapo ML, Saver JL. Cerebral microbleeds after use of extracorporeal membrane oxygenation in children. J Neuroimaging. 2013;23(1):75-78. doi:10.1111/j.1552-6569.2012.00723.x
- Jackson JC, Hopkins RO, Miller RR, Gordon SM, Wheeler AP, Ely EW. Acute respiratory distress syndrome, sepsis, and cognitive decline: a review and case study. South Med J. 2009;102(11):1150-1157.
- Kamenar E, Burger PC. Cerebral fat embolism: a neuropathological study of a microembolic state. Stroke. 1980;11(5):477-484. doi:10.1161/01.str.11.5.477
Messina MD, Levin TL, Conrad LA, Bidiwala A. Vaping associated lung injury: A potentially life-threatening epidemic in US youth. Pediatric Pulmonology. 2020;55(7):1705-1711. doi:10.1002/ppul.24755
Challa Case Report